
Graphic Design
Design Research
Dalberg Design
2021
Social Impact & Development
Miro, Adobe Illustrator
The COVID-19 vaccination program was started in early 2021, across multiple states in India, to help people reduce the severity of symptoms of contracting the coronavirus. However, several cases were being reported of people that were hesitant due to prevalent misinformation being circulated on social media about the vaccine. I worked in collaboration with Dalberg Design and the Government of Nagaland, to take part in the research process along with creating the final communication design collateral to help tackle vaccine hesitancy in Mon District, Nagaland (India).
The Context
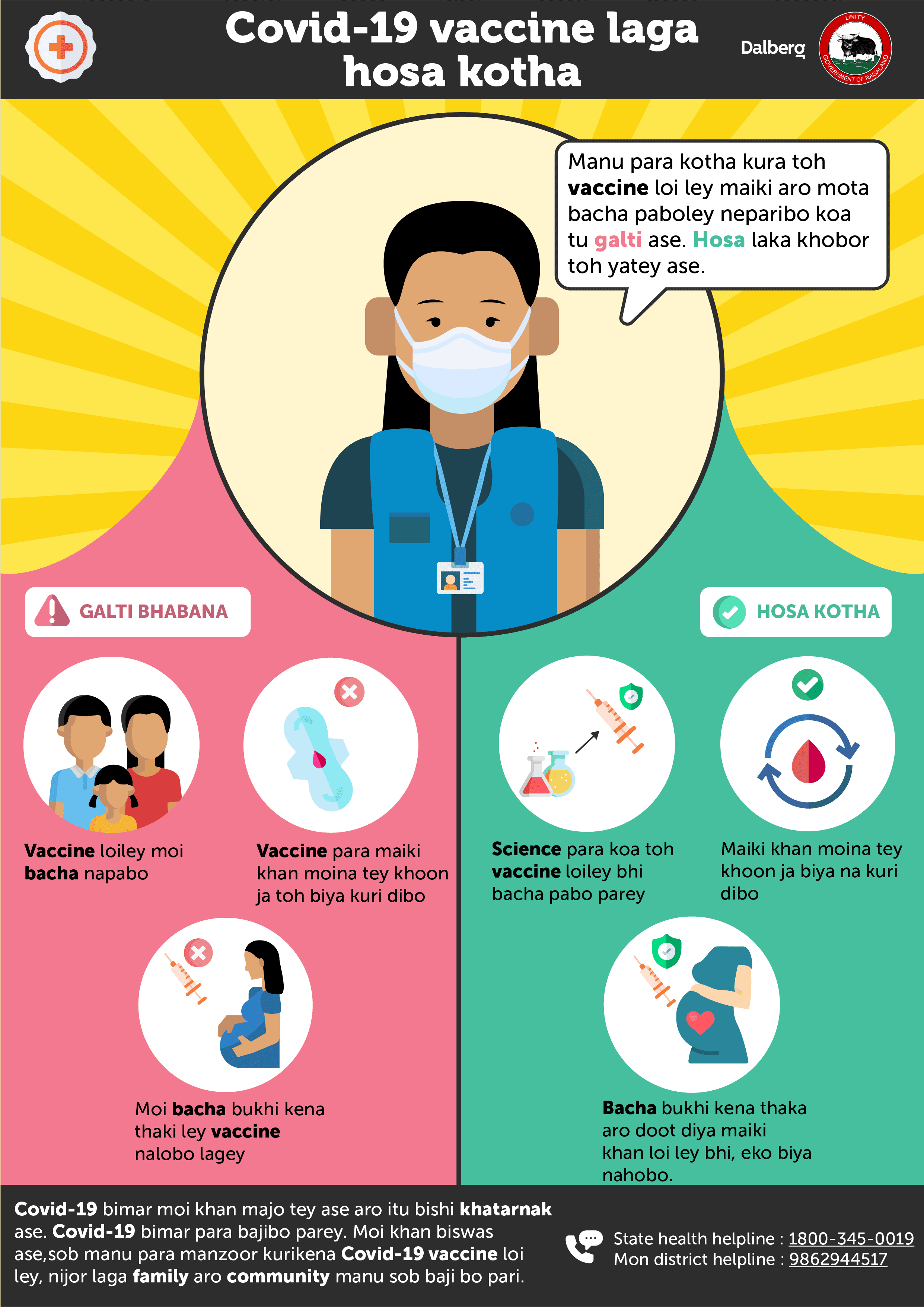
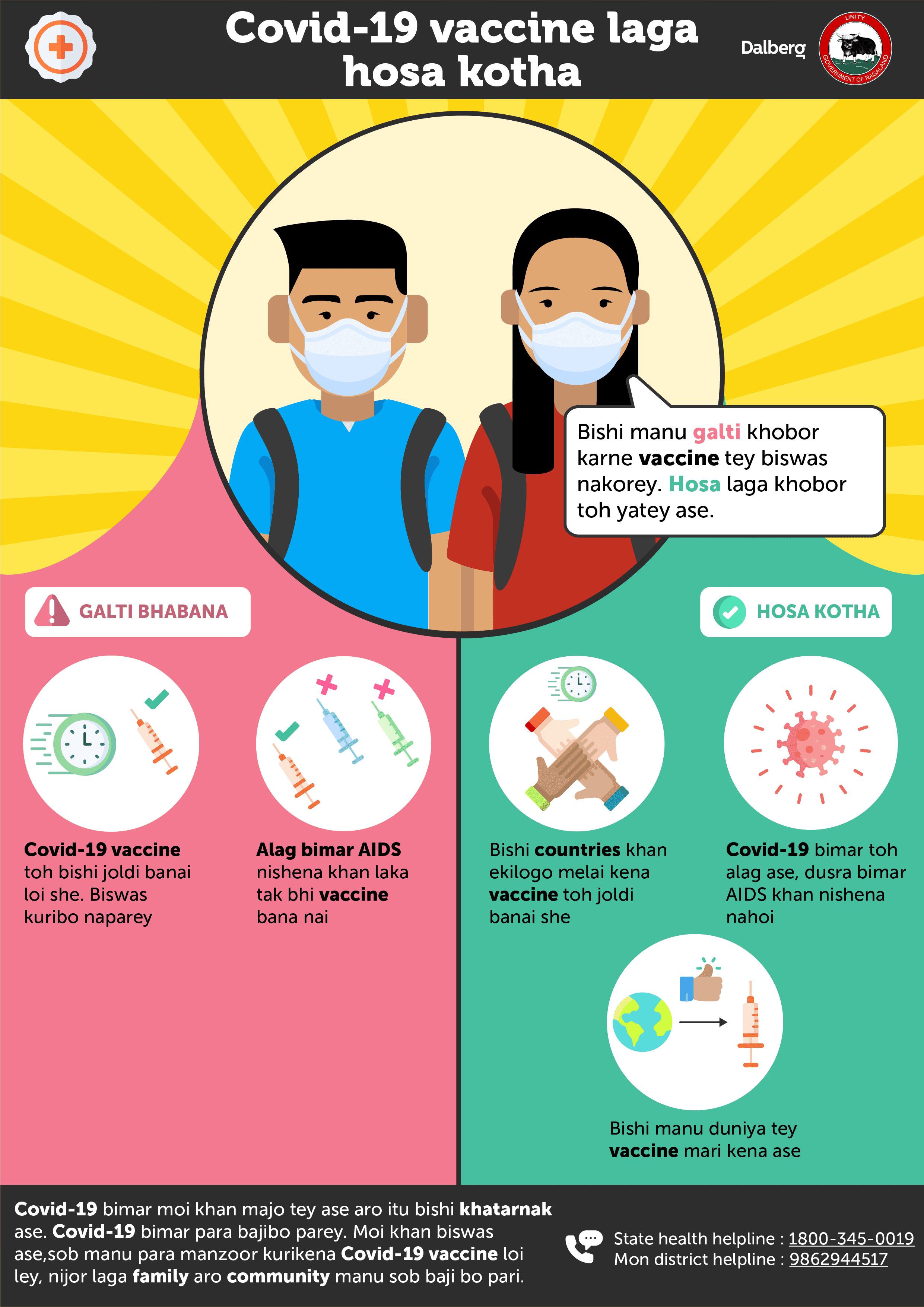
Vaccine misinformation was spreading faster than facts through WhatsApp groups in Mon District — a region with limited internet connectivity, low health literacy, and low trust in government agencies. Digital-only interventions wouldn't work. The challenge was designing something that could reach people who don't have consistent device access, don't respond to medical jargon, and weren't going to take a poster seriously if it looked like it came from the state.
What I Built
Ran 3–5 open-ended interviews per target demographic (sceptics, believers, misinformed) alongside a quantitative survey across ~100 households with on-ground government support and a Nagamese translator. Early interviews surfaced a finding that reframed the whole brief: the real barrier wasn't ignorance — it was perceived irrelevance and low emotional risk. Trust didn't come from authority, it came from familiarity.
That shifted the design direction. Five rapid prototypes were sketched, tested with a second cohort for fresh perspective, then refined into two final solutions: a lived-experience video format for ASHA workers and health officials, and a poster series for data-dark communities. My work focused on the posters — custom illustrations of locally trusted figures, copy in Nagamese and English, myth-and-fact structure designed to be read without a health worker present. Print files delivered to 10+ village health centres and markets.
Key Findings
Trust signal — People engaged more openly once a local intermediary was involved; government affiliation actively reduced participation
Gender gap — Men often controlled the household device and directed women's answers during interviews — a constraint that shaped where and how the posters needed to be placed
Distribution is the intervention — Getting the material to the right physical spaces mattered as much as the design itself
Multi-medium is necessary — Radio, posters, and peer networks together; no single channel was sufficient for behaviour change at this scale


MORE PROJECTS

